The NHS’s poor performance is no longer a funding issue but a structural one. New data reported by the Daily Telegraph shows the UK near the bottom of developed nations for treatable mortality and waiting times. Chronic underinvestment in diagnostic equipment and hospital capacity has left the system slow and constrained. This is not accidental but driven by the incentives of a tax-funded model, which prioritises short-term spending over long-term infrastructure.
Canada’s appearance at the bottom of the international rankings will surprise no one familiar with global healthcare systems. Its model is, if anything, even more constrained than the NHS – with severe capacity shortages, long waiting times and limited access to diagnostics. That the UK performs only marginally better is not reassuring. It is alarming.
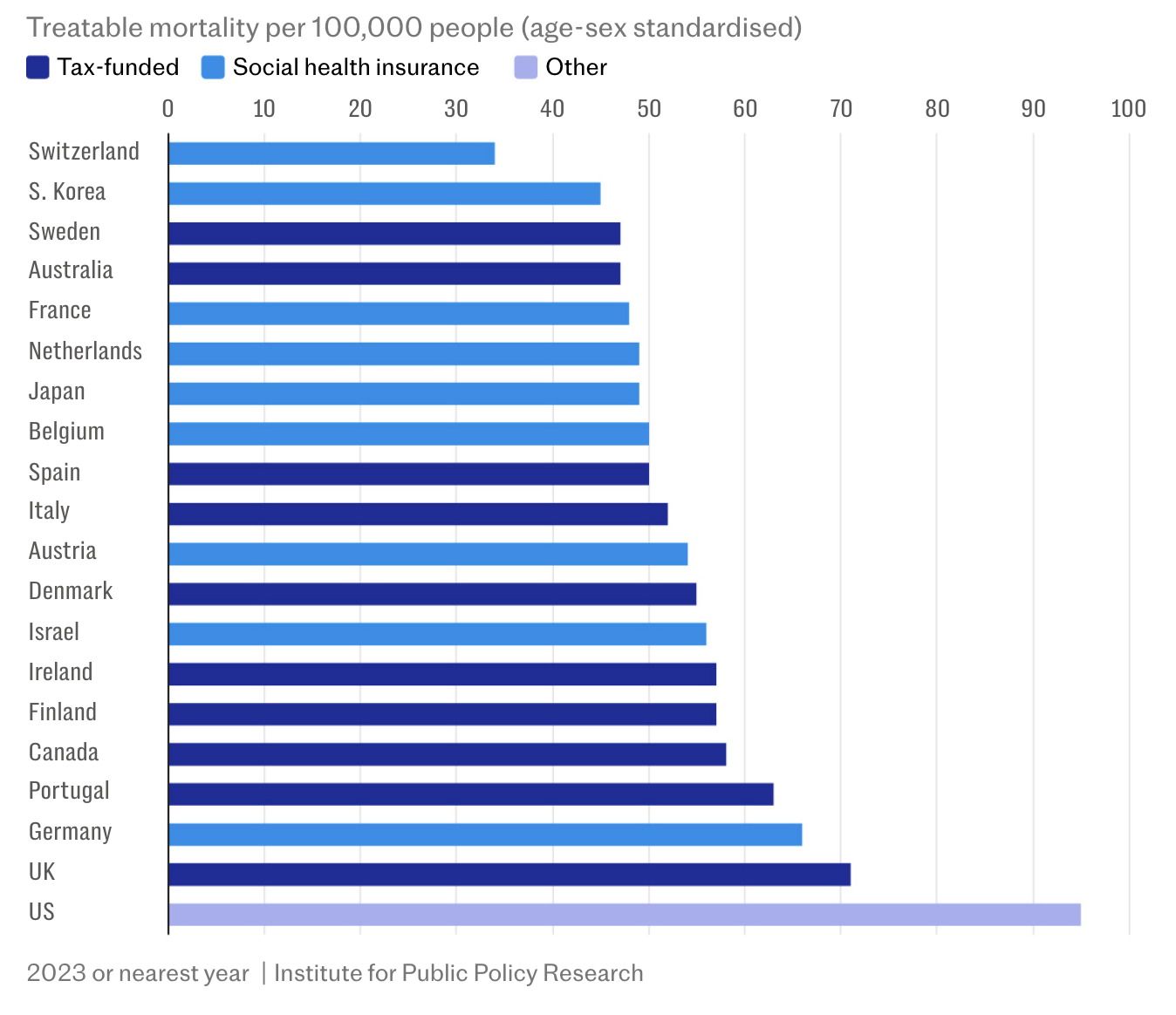
The latest analysis from the Institute for Public Policy Research, reported in the Daily Telegraph on 13 April, shows that NHS patients face some of the worst survival rates in the developed world for conditions that should be treatable. On “treatable mortality”, the UK ranks near the bottom of 22 wealthy nations, ahead of only the United States.

The data is unambiguous. Switzerland records around 34 deaths per 100,000 from treatable causes. South Korea sits at roughly 45. Germany is at approximately 66. The UK, by contrast, is closer to 71, with only the US significantly worse. This is not a marginal difference. It reflects a system that is slower to diagnose and slower to treat.

Waiting time data reinforces the point. Around 42 per cent of UK patients report waiting two months or more for a specialist appointment. In Germany, that figure is closer to 24 per cent. In Switzerland, it is nearer 14 per cent. For elective surgery, nearly half of UK patients face extended waits, compared with roughly one in five in Germany and the Netherlands. These are not isolated inefficiencies. They are systemic delays.
The report correctly identifies a core problem: the NHS lacks capacity. The UK has just 19 MRI, CT and PET scanners per million people. Comparable tax-funded systems have around 50. Social insurance systems average 68. Capital investment – in buildings, equipment and technology – remains around half that of peer countries. Fewer scanners, fewer beds and fewer treatment pathways inevitably lead to slower care and worse outcomes.
What the report understates is why this has happened.
The NHS is not simply a system where money has been “poorly targeted”. It is a system where the structure of funding makes poor targeting more likely. England’s NHS employs around 1.7 million people, with staff costs accounting for roughly two-thirds of expenditure. In such a system, political incentives are clear. Increasing pay and staffing delivers immediate, visible results. Investing in infrastructure does not.
Governments respond accordingly. Wage settlements can be announced quickly and felt immediately. New diagnostic capacity takes years to plan, procure and deploy. It delivers benefits beyond the electoral cycle. In a tax-funded system, that is a structural disadvantage.
The result is predictable. The NHS becomes labour-heavy and asset-light. It has highly trained clinicians, but insufficient tools. Doctors cannot diagnose without scanners. Surgeons cannot operate without theatre space. Patients wait, and outcomes deteriorate.
The IPPR report argues that the funding model itself is not the issue. That is only partially correct. The model may not determine outcomes directly, but it shapes the incentives that drive spending decisions. Over time, those incentives matter. They determine whether money flows into long-term capacity or short-term operational pressures.

Even the report’s claim that tax-funded systems have lower administrative costs misses the point. Administrative efficiency is not the same as clinical effectiveness. The UK may spend less on administration as a percentage of total health expenditure, but it is clearly underperforming on the outcomes that matter: speed of access, timeliness of treatment and survival rates.
This is the reality facing patients. The NHS does not lack clinical skill. It lacks timely access to care. When nearly half of patients report long waits for elective surgery and more than four in ten face delays for specialist appointments, the issue is no longer abstract. It is a capacity failure with real consequences.
For MMG, this is not an ideological debate. It is a structural market condition. The UK system cannot currently meet demand within clinically appropriate timeframes. Across Europe, however, there is available capacity – modern hospitals, advanced diagnostics and shorter waiting times.
The conclusion is straightforward. The NHS is not failing because it lacks money. It is failing because the system channels that money in ways that prioritise short-term political pressures over long-term capacity. Until that changes, patients will continue to wait – and increasingly, they will look elsewhere.
The NHS’s poor performance is no longer a funding issue but a structural one. New data reported by the Daily Telegraph shows the UK near the bottom of developed nations for treatable mortality and waiting times. Chronic underinvestment in diagnostic equipment and hospital capacity has left the system slow and constrained. This is not accidental but driven by the incentives of a tax-funded model, which prioritises short-term spending over long-term infrastructure.
Leave a Reply